
PI’s: Frank Hammond III, Brian Emling, Kinsey Herrin, Michael L. Schmitz,
Funded by: Shary and Matt Price Chair
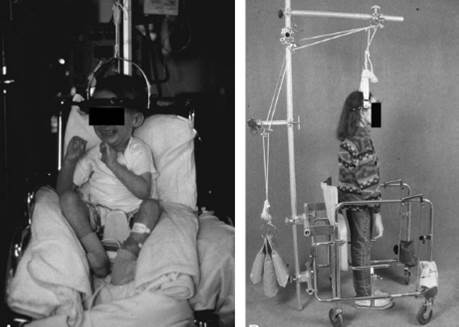
Scoliosis is a three‐dimensional deformation of the spine and has prevalence rates reported in the literature which range from 0.3%‐15.3%. When severe, and particularly when present in children of a young age, scoliosis can have significant and detrimental impacts on respiratory and heart function as well as lung, heart and chest development. Children with severe scoliosis are treated surgically with the goal of improving pulmonary function and restoring balance to their spine. Prior to surgery, weight based halo‐gravity traction is used to increase curve flexibility and reduce the risks for neurological injury. Halo‐gravity traction is reported in the literature to be a safe and effective means for applying gradual, sustained spinal traction prior to surgery in severe cases of scoliosis, kyphoscoliosis and kyphosis. While halo‐gravity traction yields successful surgical outcomes for these complex cases, it entails significant practical implementation and logistical challenges for children and their families. During halo‐gravity traction treatment, otherwise normally active children are physically tethered to a wheelchair and/or walker for 24 hours a day for 4‐6 weeks prior to their surgery. This treatment can occur in outpatient or inpatient settings and presents significant challenges to families in both scenarios due to the bulky and unwieldy size of existing halo‐gravity traction systems, which make mobility activities like sitting, lying down and age‐appropriate play impractical. Transportation is also negatively impacted due to the need to accommodate such bulky systems which do not easily fit into normal vehicles. Finally, because the current system applies traction using a static, weight based method, the magnitude of traction does not necessarily remain constant throughout a child’s treatment making consistent traction magnitude throughout treatment impossible; for example, if a child moves up in the bed while under traction, the magnitude of that traction may decrease. There is only one other investigation into altering the current method of weight‐based halo‐gravity traction, but this system still incorporates a wheelchair a walker which do not eliminate the issues associated with the size and bulk of the device. Therefore, halo‐gravity traction treatment needs to be modernized in order to provide increased normalcy for children undergoing the treatment and to allow families flexibility in their treatment arrangements.
Our research team plans to address this currently unmet clinical need by incorporating traction directly into the halo and custom back brace via a set of compression springs, rather than suspending the patient via the halo ring from an external chair or stroller for gravity traction using a weight based system. Our Halo Intrinsic Traction (HIT) system will make great strides toward easing community mobility for children during treatment as well as remove the need for limited supply wheelchairs and walkers which require inpatient stays at Children’s Healthcare of Atlanta. Furthermore, the HIT system will maintain consistent traction force throughout treatment that will be measurable and recordable throughout the process. HIT will be a significant improvement over existing systems allowing clinicians to more accurately apply and monitor traction throughout treatment.